
Do I Need To Address My Meniscus Tear With Surgery?

The following five key factors will help you and your medical team decide if you need to address your meniscus tear with surgery: where the tear is located, what caused the tear, what type of tear and how large it is, your symptoms, and finally your age and activity level. Lets review these elements below.
1. Where is your tear located?
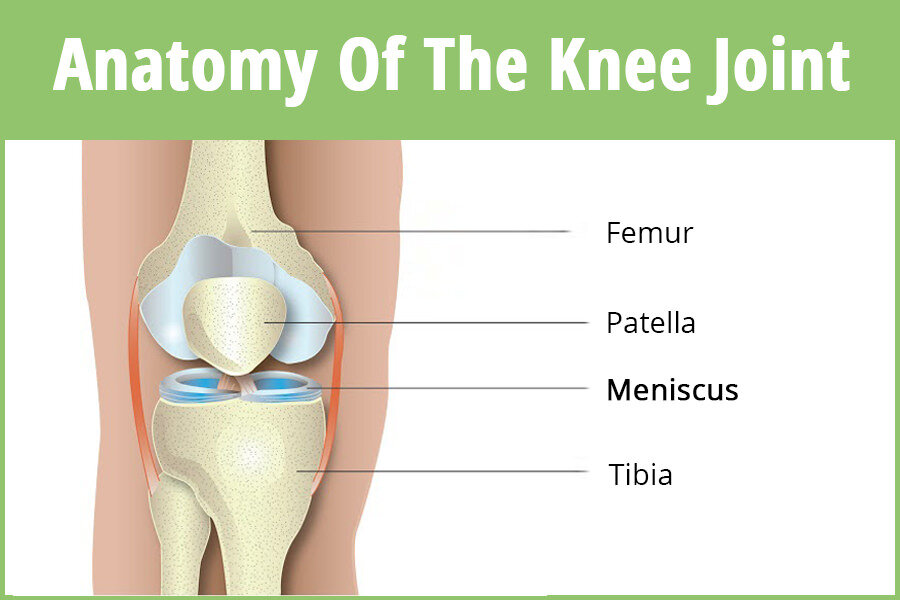
Where is the meniscus tear is located will help determine if surgery is needed. The meniscus is divided into thirds: the outer third is the "red zone" with blood supply. The inner two-thirds are the "white zone" without blood supply.

2. Was your tear caused by trauma or by degeneration?
Trauma to a meniscus typically occurs under a loaded deep knee bend or squat and a pivot or twist. You often hear a pop and experience intense pain while it's happening. Non-traumatic degenerative tears occur when many micro injuries cause wear and tear over a long period of time. Your symptoms will slowly build, involving stiffness and pain.
3. What type of tear do you have and how large is it?
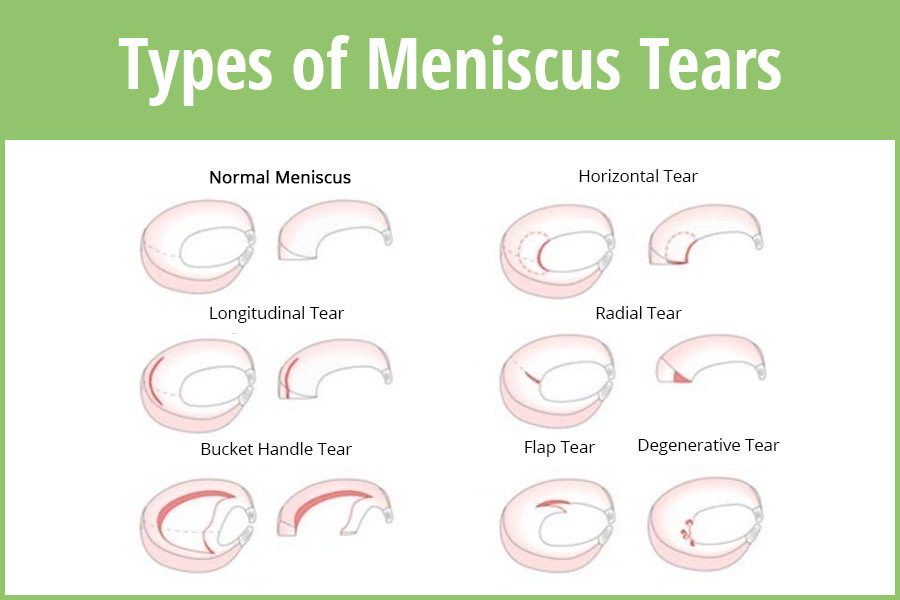
Horizontal Tears: are generally located in the white zone. They tend to heal poorly without surgical intervention. However, this type of tear can usually be repaired with a few stitches, salvaging your tissue.
Longitudinal Tears: are typically partial, stable, and located in the red zone. They rarely require surgical intervention and may not even show up on an MRI.
Radial Tears: are the most common type of tears. Since they're located in the white zone, they are difficult to heal. This type of tear usually requires surgical intervention to shave off the damaged area of tissue so you begin to heal.
Bucket Handle Tears: are large horizontal tears that fold over into the joint space. These tears are typically the most symptomatic because they limit your motion and can cause locking and buckling in the knee. Surgical intervention is required to remove the tissue that is causing the symptoms.
Flap Tears: These tears are less common. Your symptoms will most likely include a catching/snagging feeling with transitions from bent to straight positions. The catching flap can usually be surgically removed with minimal loss of tissue.
Degenerative Tears: occur when many micro injuries cause wear and tear over a long period of time. Your symptoms will slowly build, involving stiffness and pain. Small tears may respond well to surgery, but larger tears typically do not due to the amount of cartilage that needs to be removed. Loss of cartilage, your body's natural cushion, tends to accelerate arthritis in the area where the tissue was removed.
4. What are your symptoms?
If you have mechanical symptoms, the probability of surgery is higher as the change in your anatomy has already caused mechanical malfunction in your knee. These are mechanical symptoms to watch out for:
audible pops or clicks with motion
locking, catching, instability, or buckling
acute pain, swelling, and stiffness in the knee area
On the occasion that your tear is large enough that it is protruding into or outside of the joint space, and if you have mechanical symptoms (audible click, locking, buckling), the likelihood of a Baker’s cyst (swelling in the back of your knee from excess synovial fluid) is higher.
However, the great news is that usually your acute symptoms can be eased with 4-8 weeks of progressive physical therapy care, thereby avoiding surgery.
5. What is your age and activity level?
Research has shown that meniscus surgery on patients over the age of 35 without mechanical symptoms typically accelerates osteoarthritis and the need for a future joint replacement. Surgery is recommended if you are younger and more active, especially if you want to continue playing sports and engaging in high impact activities. Plus, surgery may be recommended if you continue to have pain, swelling, and mechanical symptoms for more than 6-12 weeks. Over the years, many research studies have been done, and 12 months after surgery there is no statistically significant difference between those who had 'real' meniscus surgery versus those who had the placebo surgery. There is no harm in trying physical therapy first, because even if it does not ease your symptoms it will better prepare you for your reconstructive surgery. Prehab has been known to maximize the success of recovery and rehab after knee surgery.